
%201-1.webp?width=148&height=74&name=our%20work%20(2)%201-1.webp)





Claim denial rates hit a record high in early 2026.
According to the research, prior authorization denials jumped 18% year over year. Besides, the average hospital was found to spend more than $43 per claim on rework.
For a mid-size system processing 200,000 claims annually, that math gets ugly fast.
Billing teams absorbing this aren't failing. They are running manual processes against payer rules that change faster than any spreadsheet to keep up with.
More payer portals mean more rule sets and more denials slipping through gaps. At the same time, providers must ensure every automation initiative remains aligned with HIPAA and healthcare data governance benchmarks.
What’s actually working is AI in healthcare. Not as a concept, but as specific tools wired into specific failure points. It means eligibility verification runs continuously. Coding validation that catches modifier errors before submission. Appeals automation that sorts the queue by recovery likelihood.
Hospitals using these tools report denial drops of 30–40%, and this post explains exactly how.
 Generate
Key Takeaways
Generate
Key Takeaways
- AI scores every claim by denial risk before submission, stopping revenue loss before it starts.
- Predictive analytics exposes systemic payer patterns and not just one-off claim errors.
- Automated coding and eligibility checks fix the two most common denial triggers at source.
- Health systems with AI-driven RCM report 40% fewer denials and measurably faster cash collection with healthcare billing automation.
- Successful AI adoption depends on balancing automation with HIPAA compliance and auditability.
What is Revenue Cycle Management, and Where Do Claims Actually Fail?
RCM covers every step from patient scheduling to final payment. Most billing errors don't happen at submission. They happen upstream, in registration, coverage verification, and coding, where a wrong digit or a missed authorization quietly sets a claim up for rejection days later.
| RCM Stage | Common Failure Point | What AI Fixes |
| Patient registration | Incorrect demographics, duplicate records | Flags mismatches at intake before scheduling completes |
| Insurance verification | Outdated coverage, wrong plan on file | Runs real-time checks tied to appointment schedules |
| Prior authorization | Missing approvals, expired auths | Tracks requirements per payer, alerts on expiry |
| Medical coding | ICD-10/CPT errors, unsupported modifiers | Validates against payer rules before submission |
| Claims submission | Missing fields, format errors | Pre-submission scrubbing catches gaps automatically |
| Denial management | Late appeals, lost recovery windows | Classifies denials, generates appeals, and prioritizes the queue |
Actually, manual prior authorization processes still account for extensive claim denials, despite being a documented, solvable problem that most facilities are still solving manually.
What Does A Denied Claim Actually Cost?
MGMA's 2026 benchmarking data puts rework cost at $25 to $30 per denied claim. That covers staff time and resubmission overhead. It doesn't cover the write-offs on claims that age out before anyone appeals them.
| Denial Rate | Annual Claims | Rework Cost | Estimated Permanent Write-Offs |
| 8% | 200,000 | $768,000 | $384,000+ |
| 12% | 200,000 | $1,152,000 | $576,000+ |
| 15% | 200,000 | $1,440,000 | $720,000+ |
There's a patient experience dimension too. When a billing dispute drags on, patients get confusing Explanation of Benefits statements months after care. That's often the last financial interaction they have with the hospital. It affects whether they come back.
How AI Cuts Denials: What's Actually Happening at Each Stage?
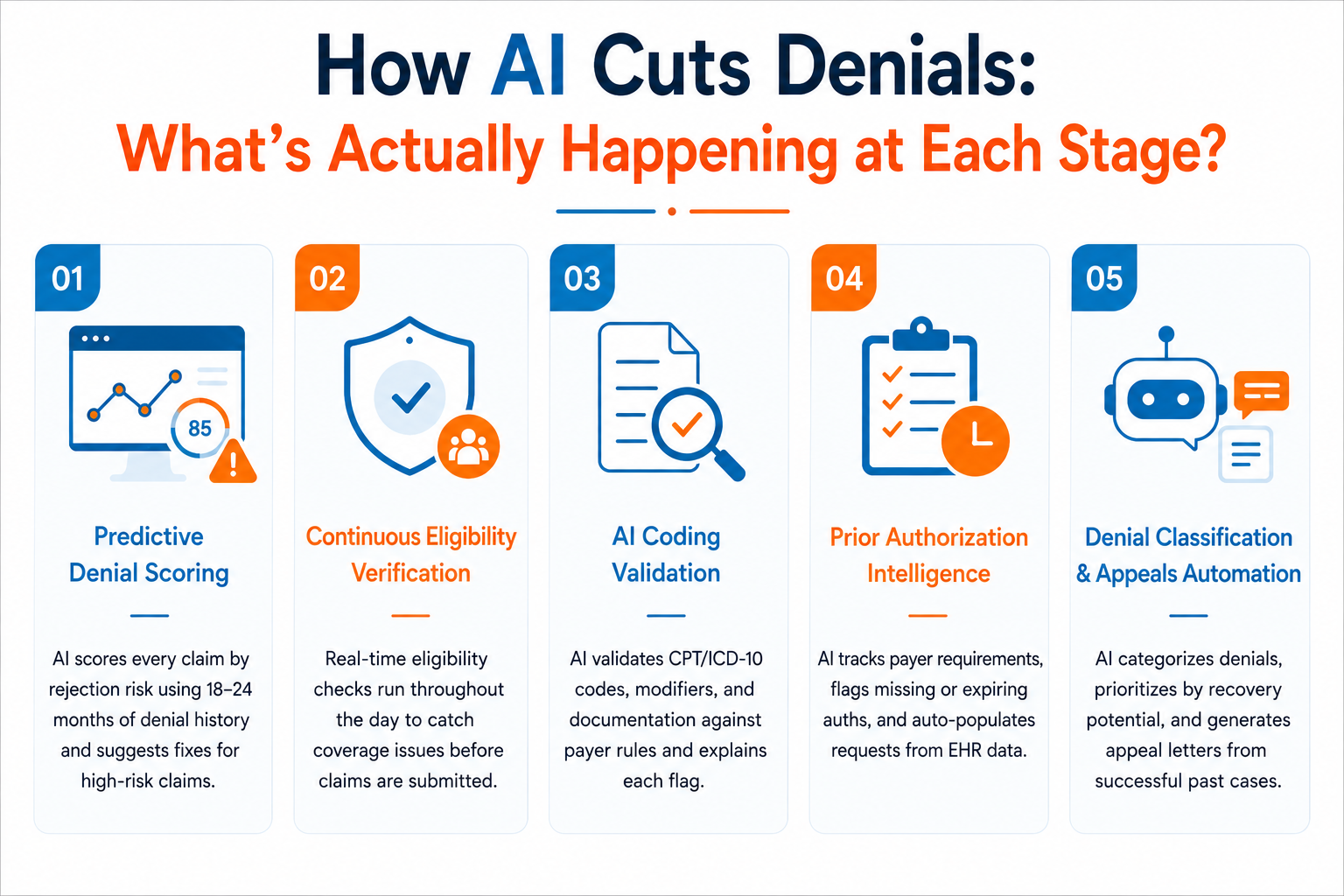
The core shift AI RCM healthcare makes possible: catch errors when fixing them is cheap (before submission), rather than after a payer has already rejected the claim. Here's where AI medical billing and RCM play out in practice.
-
Predictive denial scoring uses ML models trained on 18–24 months of a facility's own denial history to score every new claim by rejection likelihood. When a claim scores high-risk, the system surfaces the specific reason and suggests a fix.
-
Continuous eligibility verification runs checks against appointment schedules throughout the day, not just at registration. iRCM's 2026 analysis found that eligibility errors drive nearly 11.65% of the national average initial denial rate. Most of those are preventable with real-time verification.
-
AI coding validation checks CPT/ICD-10 combinations, modifier use, and documentation completeness against payer-specific rules before submission, and references the specific payer guideline behind each flag, so coders understand the reasoning.
-
Prior authorization intelligence maintains live payer requirement databases, flags missing or expiring authorizations, and auto-populates standard auth requests from EHR data. The goal is to stop approvals from falling through gaps nobody had the bandwidth to watch.
-
Denial classification and appeals automation: When denials arrive, AI categorizes them by root cause, generates appeal letters from prior successful appeals on the same denial type, and sorts the queue by dollar value and recovery probability.
What the Numbers Look Like After 12 Months of AI in RCM?
The 40% claim denial reduction figure isn't theoretical for AI in healthcare.
iRCM's 2026 client data showed an average 36% drop in denial rates at facilities using predictive tools for over a year, with the highest-denial sites hitting 40–43%.
| Source | Denial Reduction | Additional Outcomes | Timeframe |
| Dastify Solutions / Morningstar, Nov 2025 | Up to 40% | 98.5% clean-claim rate; 30–40% faster reimbursement; 2M+ claims/year | Ongoing |
| CaliberFocus Health Network / Representative case study | 35% | 12.3% → 8.0%; 120,000 fewer denials/year; $12.7M annual savings; 65% less rework | 18 months |
| Health Data Management / Peer-reviewed study | 34% | 41% reduction in days in A/R post-implementation | Post-impl. |
| CareCloud Continuum / CareCloud, Jan 2026 | ~50% fewer errors | Clean claim rates up 10–20 percentage points across client base | Ongoing |
| Experian Health AI Advantage / State of Claims 2025 | 69% of AI users | Measurable denial reduction or improved resubmission success confirmed | Annual 2025 |
Source: ircm
Results vary by starting denial rate and integration depth through AI RCM healthcare. Facilities already running low denial rates see smaller percentage drops, but the dollar recovery is often still worth the investment.
Implementation Guide: How to Phase AI RCM Without Breaking Billing Operations?
Facilities that struggle with AI RCM deployments usually try to overhaul everything at once. Those who see quick results pick one or two workflows, prove ROI, and build from there.
- Start with a denial pattern audit. Pull 18 months of data by payer and reason code. That tells you where AI moves the needle fastest in your specific environment.
- Then confirm the integration depth before signing with any vendor: a tool that reads EHR data in real time produces different results than one that runs overnight batch updates.
- Vendor evaluations should also include HIPAA safeguards, Business Associate Agreements (BAAs), encryption standards, and audit logging capabilities.
- Build a compliance review step before AI coding recommendations go live. Revenue cycle AI systems should operate under documented governance policies that define human review requirements, audit logging procedures, PHI access controls, and escalation pathways for high-risk coding decisions. Compliance and HIM teams should participate in validation before production deployment.
- AI-generated coding changes that bypass clinical review can recover claims in the short term but create audit exposure. In short, a coder reviewing flagged changes before submission isn't a bottleneck; it's a necessary check.
- Measure at 90 days. If a workflow isn't moving denial rates or cost-to-collect, reconfigure it before expanding.
Key Use Cases Across the Revenue Cycle
| Revenue Cycle Area | What AI Does |
| Patient access | Verifies coverage, catches registration errors, automates intake |
| Medical coding | Validates CPT/ICD-10, checks documentation support, flags modifier errors |
| Claims management | Scrubs before submission, monitors for missing fields |
| Denial prevention | Scores claims by risk, surfaces payer-specific patterns |
| Accounts receivable | Prioritizes follow-up by age and recovery probability |
| Financial forecasting | Projects cash flow based on denial trends and payer behavior |
How Signity Helps Hospitals Deploy AI in Revenue Cycle Management?
Signity builds healthcare AI solutions designed for how revenue cycle teams actually operate, integrated with existing EHR and billing infrastructure rather than bolted on top of it.
On the RCM side, Signity's work includes:
- Predictive denial engines trained on facility-specific payer and claim data, not generic industry models
- Real-time eligibility verification modules that connect directly to scheduling workflows and fire checks continuously, rather than at a single point in registration
- AI coding validation that references payer-specific rule libraries and explains each flag in language that billers understand, not just error codes
- Appeals automation that learns from your successful overturn history and generates appeal letters matched to your payer relationships
What sets Signity's approach apart from off-the-shelf RCM AI ROI is its integration depth. Most AI tools work well in demos and struggle in production because the EHR connection is shallow. Signity's implementations are built around HIPAA and HL7/FHIR integration from day one, with compliance review workflows built into the deployment, not added after go-live.
For CFOs and revenue cycle directors evaluating AI RCM: the question isn't whether the technology works. The data above shows it does. The question is whether the implementation fits your billing environment. That's where Signity focuses.
Conclusion
Denial rates are up, rework costs are rising, and payer requirements are not getting simpler. More importantly, billing teams running manual processes are fighting a structural problem with tools that weren't designed for this volume or complexity.
However, the hospitals seeing 30–40% claim denial reductions are not running experiments. They are using production AI tools for eligibility verification, coding validation, claim scrubbing, and appeals triage. The results show in faster collections and lower cost-to-collect.
For most revenue cycle leaders in 2026, the decision is not whether to adopt AI in RCM. It's which workflows to start with and whether the vendor can actually integrate at the depth your environment requires.

Mangesh Gothankar


Ashwani Sharma
Achin Verma
Frequently Asked Questions
Have a question in mind? We are here to answer. If you don’t see your question here, drop us a line at our contact page.
How does AI reduce healthcare claim denials?
![]()
Can AI really cut claim denials by 40%?
![]()
Which revenue cycle workflow gets the fastest payback from AI?
![]()
What is predictive denial management?
![]()
Is AI-powered RCM HIPAA-compliant?
![]()
What does AI in RCM look like in the next two years?
![]()






.png?width=352&name=agentic-ai-infrastructure-trends%20(1).png)















